
What if the simple act of forgetting one pill could change everything? For the millions of Americans caring for aging parents, that question carries a heavy weight. You’re balancing your own life while ensuring your loved one’s well-being. It’s a lot to handle.
According to the CDC, nearly 70% of people aged 40-79 use at least one prescription drug. About one in five Americans takes five or more. The more prescriptions someone manages, the harder it is to track everything. This is where a solid system becomes essential.
We created a practical, printable tool to lift this burden. This isn’t just another form. It’s a reliable partner in your caregiving journey. It helps you coordinate with doctors and pharmacies, ensuring nothing is missed.
Think about the last emergency visit. Could you recall every detail? This tool eliminates that panic. It provides the confidence and control you need. Keeping a current medication list is a lifesaving step, and it’s a core part of a comprehensive safety strategy for seniors living independently.
Key Takeaways
- A significant number of adults manage multiple prescriptions, making organization critical.
- A dedicated tracking system provides peace of mind and reduces errors.
- Having all health information in one place is vital during emergencies.
- This printable tool is designed to be simple, adaptable, and shareable with family.
- Proper organization is a key part of ensuring senior safety and well-being.
- Modern tools can work alongside traditional checklists to support caregivers.
Understanding the Importance of a Medication Adherence Checklist
Picture this: your mom is rushed to the hospital, and in the chaos, no one knows what prescriptions she’s on. This single moment shows why tracking is so vital. You are not being overprotective. You are being a smart, responsible coordinator of care.

Why Tracking Medications Matters for Caregivers
When a loved one sees several specialists, information can get lost. A cardiologist, an endocrinologist, and others may prescribe treatments without the full picture. Your accurate list becomes the bridge. It prevents dangerous combinations and ensures every provider has the correct information.
This is especially true in an emergency. If your family member cannot communicate, your list tells paramedics exactly what they are taking. This knowledge helps avoid harmful drug interactions and guides correct treatment immediately. Studies confirm that proper documentation significantly improves patient safety.
How Accurate Medication Lists Improve Health Outcomes
Getting the right medicine at the right time is what leads to real results. Blood pressure stabilizes. Diabetes stays under control. This consistent routine is only possible with a clear, shared record.
Bringing your list to appointments saves time and reduces confusion. It helps doctors make the best decisions. The emotional peace of mind you gain is priceless. It turns worry into confidence. For more support, see our long-distance caregiving guide.
| Situation | Without a Current List | With a Current List |
|---|---|---|
| Emergency Room Visit | Risk of incorrect treatment due to unknown drug history. | First responders have immediate, life-saving information. |
| Specialist Appointment | Potential for conflicting prescriptions and side effects. | Clear coordination between all healthcare providers. |
| Daily Routine | Confusion over doses and times, leading to mistakes. | Structured schedule that supports stability and well-being. |
Your effort in maintaining this list is a powerful act of love. It protects the health of someone who depends on you.
Using the Medication Adherence Checklist Effectively
Your role as a caregiver becomes much smoother when you have a clear system for tracking health information. This tool transforms overwhelming details into manageable steps.
Try JoyCalls Free
No app or new device needed. Start with a free 7-day trial.
Printable Checklist Overview and Benefits
Our printable format offers immediate organization. You can place copies where they’re needed most—near the medicine cabinet, in your wallet, and with family helpers.

The checklist creates a single source of truth. It includes space for emergency contacts, allergies, and detailed instructions for each prescription. This comprehensive approach supports better medication management across multiple providers.
Step-by-Step Guide to Tracking Medications Prescribed
Start by noting each pill’s appearance alongside its name. Your loved one might recognize their “small white pill” faster than the formal drug name.
Group medicines by health condition rather than alphabetically. This helps spot potential duplicates during doctor visits.
Update your list immediately after appointments. Take a photo of the current version for quick access on your phone. This method works well alongside modern check-in solutions for comprehensive care.
Schedule an annual review where you bring all actual bottles to appointments. This gives providers complete visibility into the treatment plan.
What Caregivers Should Do When Medication Plans Go Off Track
A Real-World Medication Plan Is Not Just About Reminders

A medication checklist is incredibly useful, but in real caregiving, the hardest moments usually happen after the checklist is made. The real pressure begins when your parent says they already took the pill but you are not sure. Or when they suddenly refuse a medication they have taken for months. Or when a hospital discharge note changes three medications at once and no one in the family feels fully confident about what the new plan actually is.
This is where many caregivers feel stuck. They may have the list, the pill organizer, the alarm, and even the pharmacy relationship in place, but they still do not know what to do when the plan starts slipping. That uncertainty is exhausting. It can make you feel like you are constantly reacting instead of calmly managing care.
The truth is that medication adherence is not only about memory. It is also about systems, observation, judgment, communication, and preparation. Seniors may miss doses for many reasons: fatigue, poor eyesight, hearing loss, side effects, embarrassment, confusion, changing routines, low appetite, cost concerns, or simple resistance to being told what to do. In many homes, the issue is not laziness or neglect. It is that the process has become too complicated for daily life.
A stronger medication system helps caregivers move from panic to response. Instead of asking, “What do I do now?” each time something goes wrong, you create a repeatable process in advance. That process should answer practical questions like:
Try JoyCalls Free
No app or new device needed. Start with a free 7-day trial.
What will we do if a dose is missed?
What signs mean the medication may be causing a problem?
Who should be called first if something changes?
How will we track medication changes after appointments?
What is our backup plan if the senior refuses help?
When these answers are decided ahead of time, caregiving becomes safer and less emotionally draining. You do not need a perfect household. You need a workable one.
A useful mindset is this: do not build a medication plan only for ideal days. Build it for stressful, rushed, confusing days too. That is what protects adherence over time.
The 5 Situations That Most Often Break Medication Adherence

Most medication breakdowns happen in recognizable patterns. If you can plan for these five situations, you can prevent a large share of avoidable errors.
1. The senior forgets whether a dose was already taken
This is one of the most common and dangerous situations because it can lead to accidental double dosing. It often happens when the day is interrupted, when medications are taken at different times, or when the senior takes them privately without telling anyone.
The best response is not to argue in the moment. It is to reduce uncertainty in the system itself. Use one clearly visible method of confirmation every single day. For example:
- mark doses off immediately after they are taken
- use a pill organizer with time-of-day compartments
- keep a simple paper log beside the medication area
- have one consistent person verify high-risk medications
- avoid storing loose tablets in multiple places
The rule should be simple: if it is not documented, it should not be assumed. That one principle can prevent many mistakes.
2. The senior refuses the medication
Refusal is often treated like a behavior problem, but it is usually a communication problem first. Seniors may refuse medication because it makes them nauseous, dizzy, constipated, sleepy, frightened, or embarrassed. Some simply dislike being controlled. Others are tired of pills and feel emotionally worn down by illness.
The most effective first step is to stay calm and get curious. Ask:
- “What feels hard about taking this today?”
- “Did it make you feel bad last time?”
- “Is the pill too big?”
- “Are you worried it is not helping?”
- “Do you want me to explain what this one is for?”
This approach preserves dignity. A senior who feels respected is more likely to cooperate than one who feels managed.
3. The medication routine changes after a doctor visit or hospital stay
This is where families get into trouble quickly. A doctor may stop one medicine, lower another, add something new, and assume the caregiver understands the whole picture. But in reality, many families go home with discharge papers, old bottles, new prescriptions, pharmacy texts, and conflicting verbal instructions.
Every medication change should trigger a same-day update ritual:
- update the medication list immediately
- circle what changed
- remove discontinued medications from the active area
- confirm pickup dates for new prescriptions
- note the reason for the change
- watch closely for symptoms during the first few days
Never rely on memory after a medication change. Write it all down while details are still fresh.
4. Side effects start but no one connects them to the medication
A senior may not say, “This medicine is causing dizziness.” They may say, “I just don’t feel right,” or “I’m more tired lately,” or “I don’t want breakfast.” That makes side effects easy to miss.
Caregivers should monitor for changes in:
- appetite
- balance
- alertness
- sleep
- bathroom habits
- mood
- confusion
- swelling
- rash
- nausea
The important part is not to diagnose at home. It is to notice patterns early and report them clearly.
5. The prescription runs out unexpectedly
This may sound small, but refill problems can disrupt the entire routine. One delayed refill can lead to skipped doses, rushed pharmacy calls, frustration, and dangerous gaps in treatment.
A refill system should never depend on someone remembering at the last minute. Build in a buffer:
- check refill status on the same day each week
- track how many doses remain for critical medications
- request refills several days early where possible
- keep pharmacy numbers visible
- know which medications should never be stopped suddenly without medical advice
A good adherence system is not only about daily use. It is also about continuity.
How to Build a Medication Escalation Plan at Home
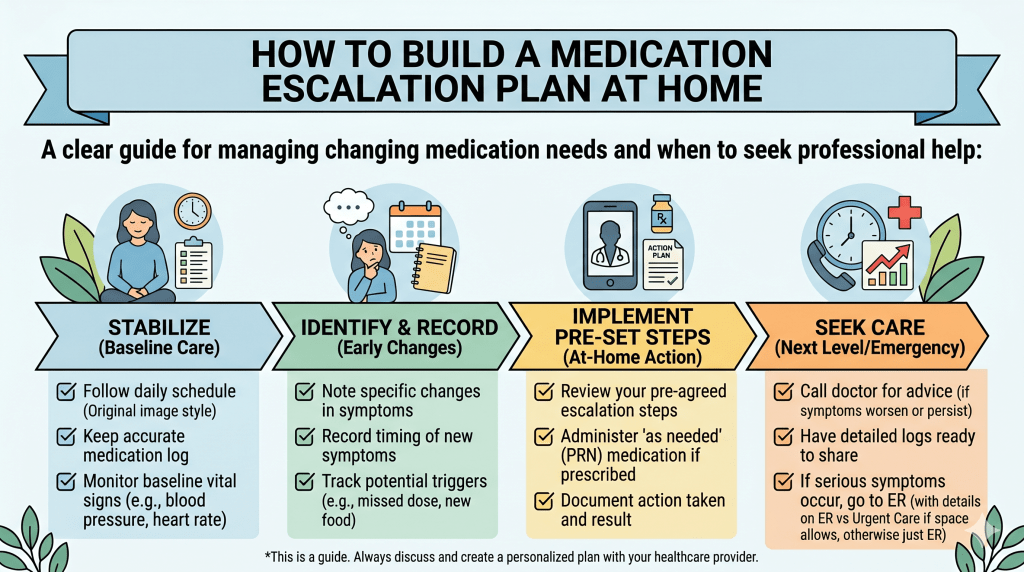
Every caregiver needs a simple home protocol for what to do when something goes wrong. This does not need to look clinical. In fact, the simpler it is, the more likely your family will follow it.
Think of it as a decision tree with three levels.
Level 1: Routine issue
Examples:
- one noncritical dose is taken late
- the senior complains about taste
- a refill is needed
- the pill organizer was filled incorrectly but not used yet
Response:
- correct the issue calmly
- document what happened
- update the checklist
- make one practical change to reduce repeat mistakes
Level 2: Concerning issue
Examples:
- repeated missed doses
- medication refusal for more than a day
- new dizziness, sleepiness, or stomach upset
- confusion about a changed prescription
- possible duplicate medicine from multiple doctors
Response:
- pause and review the medication list
- call the pharmacy or prescribing office
- document symptoms, timing, and recent changes
- do not improvise with extra doses unless explicitly instructed by a medical professional
Level 3: Urgent issue
Examples:
- difficulty breathing
- fainting
- swelling of lips or face
- severe confusion
- sudden chest pain
- signs of stroke
- suspected overdose
- severe allergic reaction
Response:
- seek urgent medical help immediately
- bring the medication list and bottles if possible
- do not waste time reconstructing the full story from memory
This type of tiered plan lowers emotional overload. Family members know whether the problem is something to monitor, something to call about, or something that needs emergency action.
The Best Way to Talk to Seniors About Medication Without Creating Resistance

One of the most overlooked parts of medication adherence is tone. A caregiver may have the best intentions, but if every interaction feels like policing, seniors may shut down. Even loving reminders can start to sound like correction when they happen every day.
That is why language matters.
Instead of:
- “You forgot again.”
- “You never listen.”
- “You have to take this.”
- “Why are you being difficult?”
Try:
- “Let’s check together so we both feel sure.”
- “I want to make this easier, not harder.”
- “Tell me what part of this routine you dislike.”
- “Would mornings or evenings feel less stressful?”
- “Let’s find a method that works for you.”
This kind of language protects independence while still keeping safety at the center.
Seniors are far more likely to follow a routine that feels collaborative. They are less likely to cooperate with a system that makes them feel watched, scolded, or incapable.
A very effective strategy is to involve them in choosing the structure:
- where should the medication station be kept?
- which reminder style feels least annoying?
- should the checklist be printed large?
- would color coding help?
- should one family member handle all medication updates?
The more ownership a senior feels, the more sustainable adherence becomes.
Create a Weekly Medication Review That Takes 10 Minutes
Many caregivers try to solve medication adherence only in the moment. But a short weekly review is what prevents the next week from becoming chaotic.
Choose one set time each week. This could be Sunday evening, Monday morning, or any quiet time that actually happens consistently. During that review, check the following:
1. Is the medication list still current?
Look for recent doctor visits, urgent care visits, specialist changes, or stopped medications.
2. Are all bottles and labels readable?
Old labels, duplicate bottles, and half-finished containers create confusion fast.
3. Is the pill organizer still correct?
Sometimes the organizer was accurate when filled, but the medication plan changed midweek.
4. Are there enough refills for the next 7 to 14 days?
Catch shortages early.
5. Have any new symptoms appeared?
Do a quick review of sleep, appetite, dizziness, mood, bowel changes, or unusual fatigue.
6. Is the current routine still realistic?
A routine that worked last month may fail now if the senior’s energy, cognition, appetite, or hearing has changed.
This weekly review does not need to become a major meeting. It just needs to be consistent. Ten focused minutes can prevent hours of confusion later.
Set Up a “Medication Command Center” That Reduces Daily Errors
One of the simplest ways to improve adherence is to create one organized place for medication management. In many homes, pills are scattered between kitchen drawers, handbags, bedside tables, bathroom cabinets, and old prescription bags. That increases the chance of missed doses, duplicate doses, and outdated medications staying in circulation.
Your medication command center should include:
- the current printed medication list
- emergency contacts
- pharmacy contact information
- prescribing doctors’ names
- allergy information
- a pen and note pad
- the current pill organizer
- a refill reminder note
- reading glasses if needed
- a small folder for medication change notes
Keep it somewhere practical, visible, and dry. Do not choose a location that is technically neat but unrealistic for everyday use.
If the senior has low vision, use:
- large print labels
- high-contrast text
- simple symbols for morning, afternoon, evening, and bedtime
- uncluttered layout with minimal visual noise
A well-designed environment quietly improves adherence because it reduces friction before mistakes happen.
What Family Caregivers Should Document Every Time There Is a Problem
When a medication issue comes up, most families remember the emotion but not the details. Then when they call the doctor, they struggle to explain what happened.
Use this simple reporting format:
What happened?
Example: “Evening blood pressure medicine was missed.”
When did it happen?
Include date and approximate time.
What symptoms did the senior have?
Be concrete: dizzy, sleepy, nauseated, confused, unsteady, not hungry.
Were there any recent medication changes?
New prescription, higher dose, lower dose, stopped drug, different brand.
What action was taken?
Called pharmacy, skipped second dose, updated checklist, monitored at home.
What happened next?
Symptoms improved, continued, worsened, or repeated.
This kind of documentation makes conversations with healthcare providers much more productive. It also helps the caregiver see patterns instead of isolated incidents.
Action Steps Caregivers Can Start This Week
To make this section genuinely practical, here are seven actions that can be implemented right away:
1. Write down your missed-dose protocol
Do not wait for a stressful moment to decide what your family will do.
2. Remove discontinued medications from active storage
Old bottles should not sit beside current prescriptions.
3. Create one visible medication log
Paper works well when multiple helpers are involved.
4. Pick a weekly refill-check day
Consistency matters more than complexity.
5. Track new symptoms for one full week after any medication change
This is when many issues first appear.
6. Use respectful, collaborative reminder language
Reduce resistance by protecting dignity.
7. Build a one-page emergency medication sheet
Keep it ready for appointments, hospital visits, and urgent situations.
The Goal Is Not Perfect Adherence. It Is Safer, Calmer Care.
Caregivers often put enormous pressure on themselves to get everything right every single day. But medication management at home is not a test of perfection. It is a process of reducing risk, noticing change early, and making the system easier to follow.
That is the real purpose of a checklist. It is not just paperwork. It is a decision-support tool. It helps caregivers think clearly when routines change, when symptoms appear, and when life gets messy.
If your current medication routine feels fragile, that does not mean you are failing. It usually means the system needs to be strengthened. With a clearer escalation plan, better documentation, more respectful communication, and a weekly review habit, medication adherence becomes more realistic and much less stressful for everyone involved.
And that matters deeply. Because seniors do not just need reminders. They need routines that respect their dignity, support their independence, and keep them safer at home.
Practical Tips and Digital Tools for Medication Management
Between your job, your family, and caring for your parent, managing prescriptions can feel like a second full-time job. The good news is that a few smart habits, combined with modern tools, can bring immense relief.
Best Practices for Medication Reconciliation and Safety
Medication reconciliation is a simple safety check. Compare the list from the doctor with what your loved one actually takes. Then, confirm it’s the correct plan. This three-way check prevents dangerous mistakes.
Your pharmacy is a powerful ally. Ask about automatic refills and 90-day supplies to avoid running out. A pharmacist can explain each drug in plain language, making the safe medication practices at home much clearer for everyone.
- Build a relationship with your pharmacist. Share your list and ask them to watch for interactions.
- Use a weekly pill organizer. It makes missed doses obvious and simplifies the daily routine.

Enhancing Adherence with Technology
For long-distance support, technology creates a vital connection. While apps and smart dispensers exist, they can be confusing for seniors.
JoyCalls offers a beautifully simple alternative. It’s an AI phone companion that makes daily calls. It gently reminds your parent about their prescriptions and asks how they’re feeling.
The best part? It requires no new technology for your loved one. It’s just a friendly voice. You receive summaries, giving you peace of mind. This daily check-in system supports consistent treatment without adding to your busy schedule.
You can sign up for JoyCalls and customize the calls to fit their specific health plan. It’s like having a caring companion there when you can’t be.
How to Build a Medication Routine Seniors Will Actually Follow
A Good Medication Plan Has to Work in Real Life, Not Just on Paper
Many medication systems look good when written down. The list is neat. The times are clear. The pill organizer is labeled. The caregiver feels prepared. But then real life happens. Breakfast is late. A doctor changes one medication. Your parent falls asleep in the afternoon. They do not feel hungry enough to take something with food. They cannot read the bottle label clearly in the evening. Or they simply decide they are tired of being told what to do.
This is where many families hit the same wall: they assume medication adherence is mostly about reminders, when in reality it is often about fit. A routine only works when it fits the senior’s energy, habits, preferences, limitations, and home environment. If the routine is too complicated, too clinical, too rigid, or too dependent on perfect memory, it will eventually break down.
That is especially important for older adults because many are already juggling multiple prescriptions, often from different providers. The article itself highlights that many adults use at least one prescription drug and that managing several medicines at once can become difficult without structure. It also emphasizes that consistency matters for emergencies, provider coordination, and daily safety.
So the goal of this section is simple: build a routine that seniors can realistically follow on ordinary days, tired days, distracted days, and difficult days.
A sustainable routine should do three things at once:
- Reduce confusion
- Protect dignity
- Make missed doses easier to detect quickly
That means the right routine is not always the most sophisticated one. Sometimes it is a printed sheet taped inside a cabinet. Sometimes it is a breakfast-linked habit. Sometimes it is one gentle phone call at the same hour every day. Sometimes it is reducing the number of decision points so the senior is not constantly trying to remember what comes next.
Caregivers often feel pressure to “manage everything.” But adherence improves more reliably when the system does more of the work. Your job is not to rely on constant vigilance alone. Your job is to create a home routine that makes the right action easier and the wrong action more visible.
Start With the Senior’s Actual Day, Not the Prescription Label Alone
A common mistake caregivers make is organizing medications around the medication list without organizing them around the senior’s real routine. On paper, a pill may say morning, noon, evening, and bedtime. But what does “morning” actually mean in that household? Is the senior up at 6:30 a.m. or 10:00 a.m.? Do they eat breakfast immediately, or only tea and toast much later? Do they nap unexpectedly? Are they sharpest in the morning or more cooperative in the evening?
Before adjusting the system, observe the pattern of a normal day:
- what time do they usually wake up?
- when do they usually eat?
- when are they most alert?
- when are they most resistant?
- what part of the house do they use most often?
- when are caregivers available?
- when do distractions usually happen?
This matters because routine beats intention. If medications are assigned to a time that does not naturally align with how the person lives, doses will be skipped, delayed, rushed, or forgotten. The article already recommends updating the list immediately after appointments and using a structured schedule that supports stability. This new section goes one step further: the schedule must be built around the person’s daily behavior, not just the bottle instructions copied into a chart.
A practical example: if a senior never reliably eats lunch, then linking a medication to lunch may create repeated inconsistency. If evenings are when confusion worsens, then a complex bedtime routine may need simplification or stronger caregiver oversight. If mornings are calm and cooperative, that is the best time to place the most important checkpoint in the day.
A medication plan becomes more effective when it follows the natural rhythm of the person’s life. That does not mean ignoring medical instructions. It means translating those instructions into a routine the household can actually maintain.
Match the Medication Routine to the Senior’s Biggest Barrier
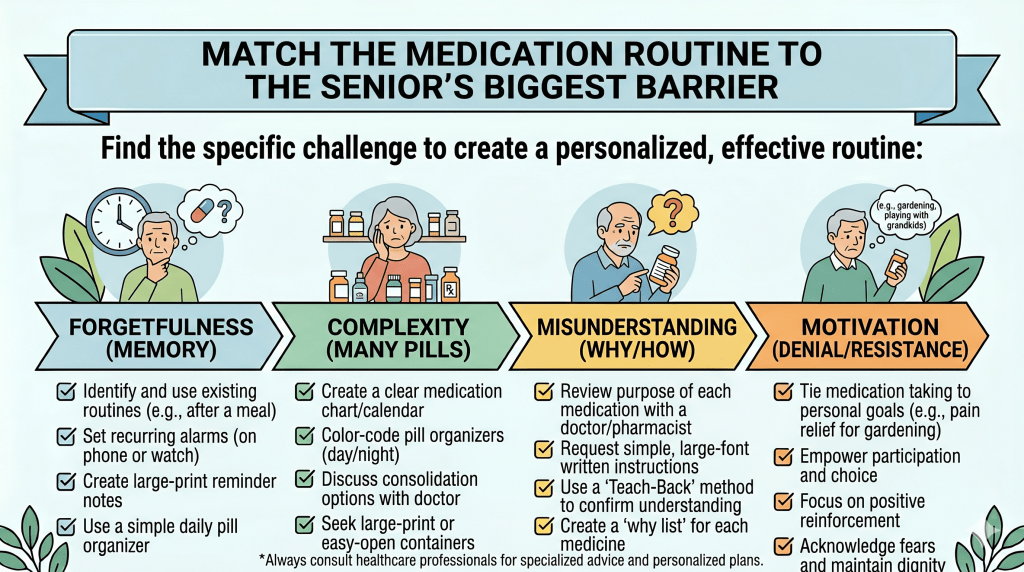
Not every senior misses medication for the same reason. That is why generic advice often falls flat. The most useful question a caregiver can ask is:
“What is the main reason this routine is breaking down?”
Usually, the answer falls into one of these categories.
Barrier 1: Poor vision
If the senior cannot read labels easily, the issue may not be memory at all. It may be access. Tiny print, similar bottle shapes, low-contrast labels, and dim lighting all increase error risk.
Helpful adjustments:
- use large-print medication lists
- keep medications in a well-lit area
- add bold time-of-day labels such as Morning, Afternoon, Evening, Bedtime
- use a pill organizer with larger compartments and clearer markings
- avoid storing medications in cluttered drawers
The current article stresses that the printable checklist can be placed where needed and that it serves as a single source of truth. For a senior with vision limitations, that “source of truth” should also be readable at a glance.
Barrier 2: Hearing issues
Some seniors miss reminders simply because they do not hear them well. App alerts, kitchen timers, or spoken instructions may not register consistently.
Helpful adjustments:
- use visual reminders instead of sound-only reminders
- place the checklist in a location they see often
- use phone calls with slower, clearer speech if calls work better than apps
- ask the senior to repeat back key instructions after appointments
- avoid giving medication instructions while the television is on
Barrier 3: Memory changes or mild confusion
When memory becomes unreliable, the system has to reduce ambiguity. The senior should never be forced to rely on recall alone to answer whether a dose was taken.
Helpful adjustments:
- use one pill organizer only, not multiple backup storage spots
- require one visible confirmation step after each dose
- keep a simple daily check-off sheet
- minimize midweek changes unless updated immediately on paper
- assign one person to refill the organizer if possible
The article already advises using a weekly pill organizer and notes that missed doses become more obvious with it. That is exactly why seniors with memory changes benefit from external cues more than verbal reassurance alone.
Barrier 4: Low appetite or nausea
Some seniors do not resist medication itself. They resist how it makes them feel. If a medication must be taken with food and the person does not feel like eating, adherence may fail repeatedly.
Helpful adjustments:
- identify which medications require food and plan around the most reliable meal or snack
- keep acceptable light-food options available if medically appropriate
- note patterns like “morning nausea” or “better tolerance after supper”
- raise recurring side-effect concerns with the pharmacist or prescriber rather than silently pushing through
Barrier 5: Emotional resistance or loss of independence
Some older adults hate the feeling of being supervised. Even when they know the medication is important, they may push back because the routine makes them feel old, dependent, watched, or incapable.
Helpful adjustments:
- offer choices where possible
- ask for their preferences about timing and setup
- avoid speaking to them like a child
- frame the routine around staying independent, not being managed
- involve them in maintaining the checklist
This is especially relevant to the article’s target audience, which centers caregivers supporting older adults while trying to preserve safety and well-being. A system that ignores pride and autonomy will often fail, even if it is medically sound.
Build a Routine Around Anchors, Not Just Clock Times

Many caregivers think in terms of exact times: 8:00 a.m., 1:00 p.m., 8:00 p.m. That may be correct medically in some cases, but in many homes, a routine tied only to clock time is harder to sustain than a routine tied to anchors.
An anchor is a consistent event in the day, such as:
- after brushing teeth
- with breakfast
- after the morning news
- before an afternoon rest
- after dinner cleanup
- before getting into bed
Anchors work because they are easier to remember than isolated times. A senior may not notice that it is 1:00 p.m., but they will notice that lunch has finished. A caregiver may forget a 9:00 p.m. alarm while driving home, but they will remember that bedtime medications go with the final evening check-in.
This method also reduces the mental burden on families. Instead of managing medication as a separate task floating outside daily life, you attach it to things that already happen.
That said, do not invent anchors that are inconsistent. If breakfast varies wildly from day to day, it may not be a dependable anchor. The best anchor is one that happens naturally and predictably.
A useful caregiver test is this: Can someone new to the household understand the routine in one minute?
If not, the routine may still be too complex.
Use “One-Step Confirmation” to Prevent Double Dosing
One of the most stressful medication moments in caregiving is hearing, “I think I already took it.”
That uncertainty creates panic because it is not always safe to guess. The article already points readers toward tools like a weekly organizer and structured tracking. To make those tools more effective, every medication system should include one immediate confirmation step right after the dose is taken.
Good one-step confirmation methods include:
- checking off the dose on a printed sheet
- flipping a time-of-day card from “not taken” to “taken”
- sending a quick text update in a shared family chat
- using a dispenser that visibly shows whether a compartment is empty
- writing initials beside the completed dose
The best confirmation step is the one the household will actually use every day. Do not choose a system that depends on multiple apps, passwords, and notifications if your household does not naturally operate that way.
This is also where caregivers can protect themselves from mental overload. When everything lives in memory, every question becomes stressful. When confirmation is visible, the system answers the question for you.
How to Reduce Medication Refusal Without Turning It Into a Daily Battle
Medication refusal is often treated like defiance, but in older adults it is usually more layered than that. They may be afraid of side effects. They may be overwhelmed by the number of pills. They may be tired of illness. They may not understand why something changed. Or they may simply resent losing control.
A refusal strategy should be calm, respectful, and structured.
First, identify the type of refusal
Is the senior:
- refusing one specific medication?
- refusing all medications?
- refusing only at one time of day?
- refusing because of side effects?
- refusing because of confusion?
- refusing only when a certain caregiver is present?
These details matter because they reveal whether the issue is physical, emotional, interpersonal, or practical.
Then, respond without escalating
Try language like:
- “Tell me what feels off about this one.”
- “Did something happen after you took it last time?”
- “Would it help if we checked the reason for this together?”
- “Let’s write down what’s bothering you so we can ask the pharmacist.”
This keeps the senior involved instead of cornered.
Finally, document patterns
If refusal keeps happening, do not just keep persuading. Track:
- which medication is refused
- when it happens
- what reason is given
- what symptoms are present
- whether a recent medication change happened beforehand
Pattern tracking makes your next doctor or pharmacist conversation much more useful.
Make Transitions Safer: After Appointments, Hospital Visits, and New Prescriptions

Medication routines become especially fragile after transitions. The live article tells readers to update the list immediately after appointments and bring actual bottles to annual reviews. That is excellent advice. The next level is to treat every medication change as a mini-reset for the whole routine.
Whenever a medication is started, stopped, or adjusted:
1. Update the active medication list immediately
Do not plan to “fix it later.” Later is when errors happen.
2. Remove discontinued bottles from the daily-use area
If old and new prescriptions sit together, confusion becomes very likely.
3. Mark what changed in plain language
Examples:
- new dose
- stop taking
- now take with food
- bedtime only
- monitor dizziness for first week
4. Inform everyone involved in care
That includes adult children, home aides, spouses, or anyone else who may help with medications.
5. Watch the first several days closely
Many side effects, timing mistakes, and tolerance issues become visible early.
Transitions are one of the biggest weak points in home medication management. A caregiver who treats transitions seriously can prevent a lot of avoidable confusion.
When the Senior Lives Alone, Simplicity Matters Even More
The article is clearly written for caregivers supporting older adults, including those who may not always be physically present. It also mentions long-distance support and positions technology as a useful bridge. For seniors who live alone, the medication routine should be even simpler, more visible, and easier to confirm from a distance.
A strong living-alone setup usually includes:
- one central medication location
- one printed list kept near the medications
- one weekly organizer
- one backup copy of the medication list in the caregiver’s phone or wallet
- one regular check-in time
- one escalation plan if the senior says they are confused or if they do not answer
What does not work well for many seniors living alone is a fragmented system: one app for reminders, another place for the list, loose bottles in multiple rooms, and no clear way for caregivers to know whether the plan was followed.
The more scattered the system, the more invisible errors become.
A Practical 7-Day Reset for Families Whose Routine Has Become Messy
If a household already feels disorganized, do not try to overhaul everything in one day. Use a one-week reset.
Day 1: Gather everything
Collect the medication list, bottles, organizer, pharmacy contacts, and doctor notes into one place.
Day 2: Confirm the active list
Compare what is on paper to what is actually being taken.
Day 3: Clean the medication area
Remove expired, duplicate, or discontinued daily-use clutter from the main routine zone.
Day 4: Rebuild the schedule around anchors
Match medications to the senior’s real daily rhythm.
Day 5: Choose one confirmation method
Pick one that everyone can follow consistently.
Day 6: Brief the whole care team
Make sure all helpers understand the system.
Day 7: Test the routine
Watch for confusion points, resistance, or timing problems and adjust while the system is still fresh.
This seven-day reset is helpful because it avoids the trap of trying to “be more organized” in a vague way. It turns medication adherence into a series of concrete household actions.
The Best Medication Routine Is the One That Reduces Friction Every Day
Caregivers often think they need more discipline when what they actually need is less friction. If the labels are hard to read, the pills are stored in three places, the instructions changed last week, and reminders feel nagging, then the problem is not motivation. The problem is design.
A better medication routine is:
- easier to see
- easier to understand
- easier to repeat
- easier to verify
- easier to update when something changes
That is what makes adherence more realistic for seniors and less exhausting for caregivers.
And that is the bigger point your article can make at this stage: the checklist is not just a document. It is the starting point for a home system that supports safer habits, calmer caregiving, and more independence for the older adult.
Because in the end, the strongest medication routine is not the one that looks the most impressive. It is the one that still works on a tired Tuesday, after a confusing appointment, when life is busy and nobody feels at their best.
How to Keep Everyone on the Same Page About Medications
Medication problems often happen between people, not just between doses
A lot of medication mistakes do not happen because someone forgot a pill. They happen because one person thought another person handled it. A daughter assumes her brother picked up the refill. A home aide follows an old printed list. A senior mentions dizziness to one family member but not another. A doctor changes a prescription, but the pharmacy still has the previous version on file. A caregiver writes something down, but no one else knows where the updated list is kept.
This is one of the biggest hidden weak points in home medication management: communication gaps.
Families often focus on reminders, pill organizers, and timing, which are all important. But even a very organized medication routine can fall apart if the people involved are not working from the same information. In many homes, more than one person touches the process. A spouse may remind. An adult child may schedule appointments. Another sibling may manage prescriptions from a distance. A pharmacist may answer questions. A physician may change a dose. A paid caregiver may help during the day. If there is no clear communication structure, everyone may be helping, but the system itself may still be fragile.
That is why a strong medication routine is not only about adherence. It is also about alignment.
When everyone involved knows:
- what medications are current
- what changed recently
- who is responsible for what
- what symptoms should be watched
- what needs to be documented
- what to do if something goes wrong
…the entire system becomes safer, calmer, and easier to manage.
This matters especially for seniors because medication management is rarely static. Prescriptions are adjusted. Specialists get involved. Hospital visits happen. New symptoms appear. Tolerance changes. The person who was managing independently three months ago may now need more support. Without a communication system, each change creates fresh room for confusion.
A caregiver does not need to create a complex medical bureaucracy at home. But they do need a simple, repeatable way to keep the right people informed. The goal is not to overcomplicate caregiving. It is to stop important details from living only in one person’s head.
Why “Informal Updates” Are Not Enough
Many families rely on casual communication:
- “I told your sister last week.”
- “I thought the doctor changed that one.”
- “I assumed the pharmacy text went to you too.”
- “Mom said she already talked about it.”
- “I didn’t realize that bottle was old.”
The problem with informal updates is not that people do not care. It is that caregiving involves too many moving parts for memory and verbal handoffs alone to stay reliable.
Informal systems usually create four recurring problems.
1. The current medication list becomes unclear
One person has a printed copy in the kitchen. Another has an older photo in their phone. The senior keeps older bottles in a drawer. A home aide follows instructions from two weeks ago. No one is completely certain which list is the active one.
2. Responsibility becomes fuzzy
When no one clearly owns a task, critical details get missed. Refill requests, follow-up calls, pickup dates, pill organizer setup, doctor questions, and symptom tracking all become “shared” responsibilities. In practice, “shared” often becomes “assumed.”
3. Information arrives in fragments
A doctor may tell the patient one thing, the caregiver another, and the after-visit summary something slightly different. The family hears pieces, but no one consolidates them into one updated plan.
4. Stress increases for everyone
When communication is loose, caregivers spend mental energy rechecking everything: Did the medication change? Was the refill requested? Did anyone monitor the side effect? Was the dose already taken? That uncertainty becomes exhausting over time.
A family communication system solves these problems by turning scattered updates into one shared structure.
The 4-Part Communication System Every Caregiving Family Should Build
A workable medication communication system does not need to be fancy. It just needs to be clear. The most effective systems usually have four parts:
1. One current medication record
There should be one place that everyone recognizes as the official, current medication record. That may be:
- a printed sheet in the home
- a shared family note
- a clearly dated spreadsheet
- a care binder
- a simple shared digital document
The format matters less than the rule: only one version is the master version.
That record should include:
- medication name
- dose
- when it is taken
- what it is for
- special instructions
- prescribing provider
- recent changes
- allergies
- pharmacy contact information
The mistake many families make is keeping several “pretty close” versions. That creates risk. Close enough is not safe enough when medications are involved.
2. One task owner for each medication-related responsibility
Medication support includes many different tasks:
- updating the active list
- requesting refills
- picking up prescriptions
- filling the pill organizer
- bringing the list to appointments
- asking doctor questions
- tracking new symptoms
- confirming discontinued medications are removed
Do not assign all of these vaguely to “the family.” Assign them specifically.
For example:
- Daughter A updates the medication list after appointments
- Son B handles pharmacy pickup and refill monitoring
- Spouse checks the printed list daily
- Home aide notes symptoms and missed doses
- One person reviews changes every Sunday evening
Specific ownership reduces dropped details. It also lowers resentment because people know what they are actually responsible for.
3. One communication channel
Medication updates should not be scattered across texts, memory, paper scraps, and random calls. Pick one primary communication channel for medication-related updates. That might be:
- one family group chat
- one shared note
- one WhatsApp thread
- one care notebook in the home
- one weekly caregiver call plus written follow-up
This becomes the place where changes are logged in a simple, consistent way.
Examples:
- “Metformin reduced today from 1000 mg to 500 mg at dinner.”
- “Refill requested for blood pressure medication, pickup Friday.”
- “Complained of dizziness after evening dose—watch tomorrow.”
- “Old antibiotic discontinued and removed from kitchen cabinet.”
The goal is not constant messaging. It is organized messaging.
4. One escalation rule
Caregiving families work better when everyone knows what kind of issue should be:
- documented only
- sent to the family channel
- phoned to the main caregiver
- called into the doctor or pharmacist
- treated as urgent
Without this, people either underreact or overreact. One sibling panics over every small symptom. Another says nothing until three doses have been missed. A simple escalation rule keeps the response balanced.
How to Divide Medication Responsibilities Without Creating Family Drama
Medication management can create tension in families very quickly. One person may feel they are doing everything. Another may help but in a way that creates more confusion. Someone may live far away and want updates, but not be involved in the daily work. Someone else may question decisions without actually taking on tasks.
The best way to avoid this is to divide responsibilities based on capacity, proximity, temperament, and consistency, not guilt.
Ask practical questions:
- Who is nearby?
- Who is good at details?
- Who is calm in appointments?
- Who can reliably follow through?
- Who communicates clearly?
- Who has time for refills and pharmacy coordination?
- Who has the best relationship with the senior?
Do not assign responsibilities based purely on family hierarchy or who feels the most emotional pressure. The “most worried” person is not always the best person for every task. The best system uses people where they are strongest.
Here is an example of a smart division of roles:
The coordinator
Keeps the master medication list updated and sends major changes to the family.
The pharmacy point person
Handles refill requests, pickup tracking, and pharmacy questions.
The appointment companion
Brings the medication list, asks clarifying questions, and confirms changes in writing.
The daily observer
Notices side effects, missed doses, appetite changes, or resistance patterns at home.
The backup helper
Steps in when the main caregiver is unavailable.
This kind of structure turns vague support into real support.
What to Communicate After Every Appointment
Appointments are one of the highest-risk times for medication confusion. A provider may change a dose casually, mention side effects to monitor, or assume the family already understands a new plan. If no one captures that information clearly, the household may continue following the old routine.
After every appointment, someone should communicate five things to the rest of the care circle:
1. What changed
Was something added, stopped, reduced, increased, or moved to a different time?
2. Why it changed
This matters because families follow through better when they understand the reason.
3. When the change starts
Immediately? After finishing the current bottle? After pharmacy pickup?
4. What should be monitored
Examples: dizziness, blood pressure, swelling, appetite, sleepiness, stomach upset.
5. What the next step is
Examples: refill today, call in one week, lab work next month, watch symptoms for three days.
A strong caregiver habit is to send this update in plain language on the same day as the appointment. Not tomorrow. Not when things calm down. Same day.
For example:
“Doctor stopped the old sleep medication today. New plan is half-dose for 5 nights, then stop. Watch for daytime grogginess and confusion. I updated the printed list and removed the old bottle from the active tray.”
That kind of message prevents three days of misunderstanding.
How to Talk to Doctors and Pharmacists More Effectively
Many caregivers leave appointments or pharmacy calls with more uncertainty than they had before. Not because professionals are unhelpful, but because families do not always know what to ask or how to summarize the problem clearly.
A better medication conversation starts with preparation.
Before you call or attend an appointment, be ready to answer:
- what medication is involved
- what the current dose is
- what changed recently
- what symptoms you are noticing
- when the issue began
- whether doses were missed or taken differently
- whether there are duplicate bottles or conflicting instructions at home
The clearer your summary, the better the response you are likely to get.
Instead of saying:
- “She’s not doing well on her medicines.”
Try:
- “Since the dose increase three days ago, she has been more sleepy in the afternoon, has eaten less, and refused the evening dose once. No falls, but she seems less steady.”
That is specific, useful, and actionable.
You should also feel comfortable asking direct questions such as:
- “Can you confirm the active dose?”
- “Should we stop the old bottle now?”
- “What side effects should we watch first?”
- “Does this need to be taken with food?”
- “What should we do if a dose is missed?”
- “Can you review this against the full medication list?”
Pharmacists are especially underused by families. They can often clarify instructions, timing, interactions, refill logistics, and label confusion faster than people expect.
The Importance of a Written Handoff When More Than One Person Helps
If more than one person helps with medications, you need a written handoff process. This matters in homes with:
- rotating adult children
- hired caregivers
- weekend helpers
- respite coverage
- long-distance family support
- hospital discharge transitions
A written handoff does not need to be long. It just needs to answer:
- What is the current medication plan?
- What changed recently?
- Were any doses missed today?
- Were any symptoms noticed?
- Is any refill needed?
- Is anything unclear and waiting for provider guidance?
A simple handoff note can prevent avoidable errors when care shifts from one person to another.
For example:
Today’s notes
- Morning meds taken
- Lunchtime dose taken late at 2 p.m.
- New swelling in ankles noticed
- Refill needed for thyroid medication by Thursday
- Waiting for callback from doctor about dizziness
This is especially valuable when the next caregiver is stepping into the day without full context.
How to Create a “No Surprises” Medication Culture at Home
The healthiest caregiving systems are not the ones where everything is always perfect. They are the ones where people say things early.
A “no surprises” medication culture means:
- people report missed doses without fear
- side effects get mentioned early
- confusion is admitted quickly
- no one pretends to understand a new instruction if they do not
- old medication bottles are not quietly left in rotation
- concerns are written down instead of brushed aside
This matters because shame and silence are dangerous in caregiving.
A spouse may hide a missed dose because they feel guilty. A hired aide may not mention refusal because they worry it reflects badly on them. An adult child may stay quiet about not understanding the discharge instructions because they do not want to look careless. These are human reactions, but they make medication management riskier.
A good caregiver leader makes it easy for people to speak up by saying things like:
- “Please tell me if anything feels unclear.”
- “I’d rather hear about a missed dose right away.”
- “If you notice a change, even if you’re not sure it matters, write it down.”
- “It’s okay not to know—just let me know.”
That kind of tone makes the whole system stronger.
The Weekly Medication Communication Check-In
Families do better with one short weekly communication review than with random stress-driven updates all week.
This review can be 10 to 15 minutes. It can happen by phone, at the kitchen table, or in a group message. It should cover:
Current plan
Is the medication list still correct?
Changes
Any new prescriptions, stopped drugs, side effects, or provider instructions?
Supplies
Any refills due soon? Any pharmacy issues?
Symptoms
Any patterns with dizziness, sleep, appetite, bowel changes, mood, confusion, or refusal?
Responsibilities
Does anyone need help with pickup, appointments, or documentation?
Risks
Any known weak spots this week, such as travel, schedule changes, or caregiver absences?
This weekly review keeps the system current without requiring constant high-intensity communication.
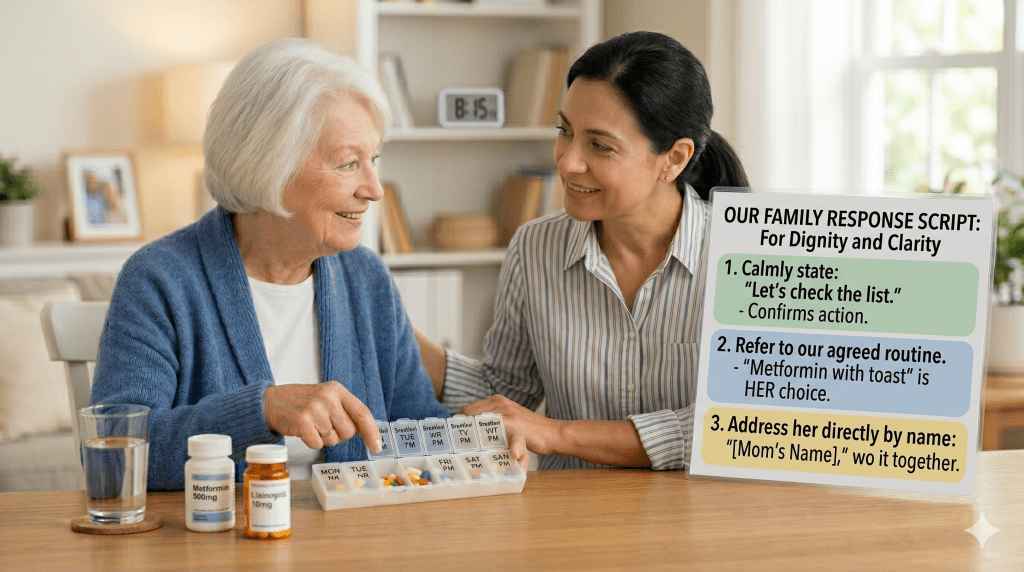
A Practical Caregiver Script for Medication Updates
Sometimes the hardest part is not knowing how to phrase things. Here is a simple structure families can use for medication updates:
Medication update
- What changed:
- When it changed:
- What we need to watch:
- What action is needed:
- Who is handling it:
Example:
Medication update
- What changed: Blood pressure medicine reduced from full tablet to half tablet
- When it changed: Started tonight
- What we need to watch: Dizziness, headache, low energy
- What action is needed: Pick up new refill on Friday
- Who is handling it: Meera updating the printed list, Raj picking up medication
That kind of structured update makes caregiving communication dramatically easier.
Highly Actionable Steps You Can Put in Place This Week
If you want this section to be immediately useful to readers, here are practical actions caregivers can start right away:
1. Choose one master medication record
Decide today which version is the official one.
2. Assign one owner to each medication task
Stop leaving refill checks, updates, and pickups vaguely shared.
3. Create one family communication channel for medication updates
Do not scatter critical information.
4. Use same-day appointment summaries
Write and send medication changes while they are fresh.
5. Start a written handoff note if multiple people help
Even a half-page note is better than memory.
6. Schedule a weekly 10-minute medication review
Short, regular reviews prevent bigger confusion later.
7. Normalize speaking up early
Tell everyone involved that uncertainty should be reported, not hidden.
Good medication care is a team process, even in a small family
Caregivers often carry a private burden of feeling that they alone must remember everything, catch everything, update everything, and prevent every mistake. But medication management becomes more sustainable when it is treated as a team process with clear communication instead of a private mental load carried by one exhausted person.
That does not mean every family member must do the same amount. It means the people involved should be working from the same plan.
A senior is safer when:
- the medication list is current
- responsibilities are clear
- updates are shared promptly
- symptoms are documented
- providers get accurate information
- helpers know when to escalate concerns
This is one of the most practical ways to reduce medication stress at home. Not by adding more reminders alone, but by making sure everyone connected to the care plan is seeing the same picture.
And in caregiving, that kind of clarity is not just organization. It is protection.
Conclusion
Taking that first step to get organized is a powerful act of love. You’ve shown incredible care by seeking out ways to better support your family member. Remember, you’re not alone in this journey.
Your healthcare providers want to help. Don’t hesitate to reach out between visits if challenges arise. Research shows that addressing concerns early leads to better outcomes. Small adjustments can make a big difference in your loved one’s treatment.
Consider combining your new system with supportive technology. Tools like daily check-ins provide peace of mind without adding stress. Studies confirm that simple reminders significantly improve consistency.
You’re doing important work. Celebrate each small victory along the way. Your dedication creates a safety net that protects health and preserves independence.