
“Did Mom eat today… or did she just think she did?” That single question can stop your day.
Nearly one in four older adults miss a meal on any given day. This is more common than many families expect.
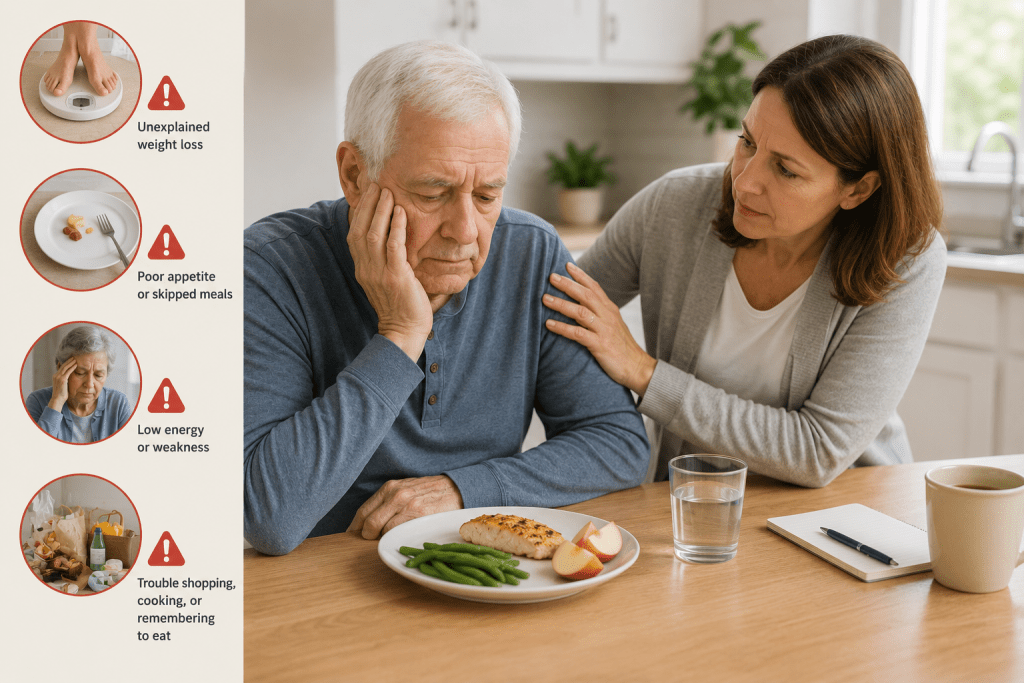
When dementia forgetting to eat shows up, it looks like missed meals, half-eaten plates, repeat questions, or sudden weight loss. A person might not recognize food, lose hunger cues, or feel overwhelmed by the routine.
Brain changes in memory, attention, vision, judgment, and taste can make eating confusing or tiring. But calm routines, steady hydration, and small prompts can help a person enjoy food again.
This guide will explain common reasons, red flags, quick checks, and gentle fixes you can try today. We won’t prescribe a special diet. Instead, we’ll focus on consistent, balanced nutrition that protects strength, mood, and immunity.
If you can’t be there every meal, think of JoyCalls as a backup set of eyes and ears. Sign up for JoyCalls: https://app.joycalls.ai/signup or talk to Joy now: 1-415-569-2439 for daily check-ins and peace of mind.
Key Takeaways
- Missed meals often stem from memory and attention changes, not stubbornness.
- Look for signs like half-eaten plates or sudden weight loss.
- Simple prompts and calm routines support regular meals and hydration.
- Balanced nutrition helps protect overall health and strength.
- Caregivers can use phone reminders or services like JoyCalls for support.
Why dementia changes eating and mealtimes
What used to feel simple—sitting down and eating—can become a multi-step challenge. The brain loses some of its meal-time autopilot. Tasks that once ran in the background now need focus. That makes a routine meal feel like a list of unfamiliar steps.

Memory and recognition
A person may not recognize a fork, plate, or cup. They might sip from a bowl or use a spoon like a fork. This is not stubbornness. They’re not being difficult—this task is difficult.
Too many choices and overwhelm
A full plate can feel like a crowded to-do list. In middle and later stages, fewer options often calm them and increase intake. Simple plates and one course at a time help the brain focus.
Reduced taste and smell
Food that once delighted can suddenly “taste like nothing.” Changes in smell and flavor blunt appetite. Favorite meals may no longer trigger interest, even for people living with memory loss.
Low energy, mood, and agitation
Low energy or depression can cut appetite. Depression affects many living with Alzheimer’s and often lowers food interest.
Try JoyCalls Free
No app or new device needed. Start with a free 7-day trial.
Agitation rises when meals are rushed, noisy, or unpredictable. A calm routine and predictable time and place help reduce stress and support eating.
- Keep plates simple.
- Offer one food at a time.
- Allow extra time and gentle prompts.
| Problem | What it looks like | Quick fix |
|---|---|---|
| Recognition loss | Uses utensils oddly; won’t touch food | Show one item at a time; hand-over-hand help |
| Overwhelm | Pushes food away; refuses choices | Serve fewer items; single-course meals |
| Taste changes | No interest in favorites | Try stronger flavors or warm foods |
| Mood/low energy | Skips meals; less movement | Small, frequent snacks; gentle encouragement |
Nutrition and hydration issues can quickly become health risks. For signs and practical mealtime tips, see a helpful guide on mealtime care and a sample caregiver check-in schedule.
Red flags and health risks when someone isn’t eating enough
Small changes can hide serious trouble. If clothing fits more loosely or energy drops, act sooner rather than later.

Unintentional weight loss, malnutrition, and weakened immunity
Unplanned weight loss in older adults raises the risk of worse outcomes, including higher mortality. Losing pounds often means losing muscle and resilience.
Malnutrition risks: weaker immune system, slow wound healing, falls, anemia after weeks, and less strength for daily tasks.
Dehydration checks caregivers can do at home
- Look for minimal or dark urine and fewer bathroom trips.
- Notice dry mouth, lightheadedness, or a rapid heart rate.
- Watch for fatigue, dizziness, and constipation.
| What to watch for | What it may mean | Immediate step |
|---|---|---|
| Looser clothes, steady weight loss | Muscle and strength loss | Track weight; add nutrient-dense snacks |
| Dark urine or very low output | Dehydration risk; UTI or kidney stress | Offer small sips often; seek care if worse |
| New confusion or agitation | Worsened brain symptoms from poor intake | Note timing; call clinician if sudden |
Behavior changes that may worsen with poor nutrition
Poor food and fluid intake can make people more confused, irritable, and restless. Track patterns for a few days, not just one meal.
Don’t wait—if they skip a full day or two of eating drinking, call a clinician. Fainting risk and serious complications rise quickly.
“If you see rapid weight loss or severe thirst, get help today.”
Next, we’ll pinpoint why this happens and what to look for.
Dementia forgetting to eat: the most common reasons (and what to look for)
Meals can be missed not because someone won’t eat, but because the steps around a plate feel unknown.
Forgetting they haven’t eaten or believing they already ate
Classic signs include insisting breakfast happened, seeming genuinely surprised when offered food, or asking if they already finished minutes later.
Try JoyCalls Free
No app or new device needed. Start with a free 7-day trial.
Not knowing what to do with food placed in front of them
Sometimes the food is visible, but the brain won’t link the steps: pick up, scoop, chew, swallow. This apraxia-like pattern leaves a full plate untouched.
Trouble using utensils or using them incorrectly
Watch for odd grips, cutting on the wrong side, or giving up in frustration. These moments often look like resistance but are skill breakdowns.
Dental pain, poor-fitting dentures, and dry mouth
Clues: jaw-touching, wincing, avoiding crunchy items, tiny sips, or bad breath. If dentures slip or hurt, a person may refuse many foods.
Medication side effects and new dosage changes
Appetite shifts often follow a new pill or dose change. If you notice new symptoms after a refill, call the clinician rather than “power through.”
Quick checklist for caregivers:
- Did they insist they already ate?
- Is food on the plate but untouched?
- Are utensils handled oddly or dropped?
- Any jaw pain, dentures issue, or dry mouth?
- Any recent medication changes?
| Cause | What you may see | Care action |
|---|---|---|
| Believes they ate | Insists meal happened; repeats the question | Offer small, familiar snack; note timing |
| Apraxia-like steps | Food present but not used | Hand-over-hand help; single-item servings |
| Utensil trouble | Wrong grip; frustration | Try adaptive utensils; simplify plate |
| Dental/dry mouth | Wincing; avoids crunchy food | Dental check; offer moist, soft foods |
| Medications | New appetite change | Review meds with prescriber |
They’re not stubborn—something is getting in the way. Check the mouth after meals if pocketing is possible, and track patterns so you can tell the clinician what you observed.
Quick caregiver assessment before changing the diet
Before swapping textures or adding supplements, pause and look for simple medical or situational causes.

Rule out pain, constipation, infection, or other medical conditions
Start with a short check. Look for common hidden conditions like constipation, urinary tract infection, mouth sores, gum disease, or ill-fitting dentures.
Medicines can cause appetite loss. Pain they can’t explain also reduces intake. A person may grimace when chewing or press their belly.
Track patterns by time of day, activities, and environments
Keep a 3–7 day log. Note the time each meal is best, where they sit, noise level, who is present, and which foods work.
Record activities before meals. A short walk or light chores may help. Fatigue often worsens appetite later in the day.
When to involve a doctor, registered dietitian, or dentist
Call a doctor if you see rapid weight loss, dehydration, choking, or sudden confusion spikes. Seek dental care for jaw pain, loose dentures, or persistent mouth pain.
Ask a registered dietitian about simple, nutrient-dense snack plans and safe calorie increases that don’t feel like pressure.
- Pause and assess before changing a diet.
- Watch for signs: fewer bowel movements, grimacing, sudden confusion.
- Log time, activities, and which foods succeed.
You don’t have to figure this out alone. For a practical assessment and checks you can use now, see this concise clinical checklist: mealtime assessment guide.
Set up a calm eating environment that helps the brain focus
A quiet, predictable dining spot can make a big difference for someone who finds mealtime confusing.

Limit distractions
Turn off the TV, mute phone alerts, and lower background noise. A simple soundscape helps the brain follow one task at a time.
Keep the setting simple
Remove centerpieces and extra condiments. Use plain tableware so the plate and foods are the focus.
Lighting and contrast
Bright, even light and a contrasting plate make food easier to see. Try a solid placemat and avoid busy patterns.
Serve one thing at a time and allow plenty of time
Offer the main course first, then sides. Limit choices to two at most. Let the person take their time—meals may take up to an hour.
Caregiver-ready checklist
- TV off and phones away
- Minimal distracting talk; consistent chair and routine
- Solid placemat and a contrasting plate
- One course at a time; two choices max
- Allow slow pace; move location if a favorite chair helps
| Goal | What to do | Why it helps |
|---|---|---|
| Make mealtimes easy on the brain | Quiet room, simple tableware | Reduces overload and supports focus |
| Improve visibility | Bright light, contrasting plate | Food stands out and is easier to pick up |
| Reduce overwhelm | One item at a time; familiar routine | Less choice lowers stress and increases intake |
“A calm table can feel like a hug.”
For more tips on making calls and check-ins feel like real connection, see how to make phone calls feel less like. Small changes help people living with memory and attention changes enjoy a meal and protect their health.
Make eating easier with the right foods, textures, and tools
A few simple swaps in texture and tools can restore confidence at the table.

Our aim is dignity: help a person eat with less frustration and more comfort.
Practical food prep
Cut foods into quarter-size bites (about the size of a quarter). Remove bones, toothpicks, garnishes, and any non-edible bits.
Finger-first mini meals
Offer finger snacks: cheese cubes, small sandwiches, chicken strips, fish sticks, sliced fruit, and steamed veggie wedges. These work well for roaming or short attention spans.
Simple tools that help
- Use a plate with a rim and non-slip mat for stability.
- Choose spill-resistant cups and mugs with lids.
- Offer one utensil only and large-handled spoons when needed.
Gentle prompting and help
Use single-step cues: “Scoop.” Pause. “Bring it mouth.” Model the action calmly. For hand-over-hand, ask permission, then guide the person’s hand through the motion with slow, respectful touch.
Don’t fight the mess. Protect clothing, focus on nourishment, and keep independence when possible. For more meal planning and clear tips, see this eating well guide.
Prevent choking and support swallowing in later stages
Swallowing changes can quietly make meals unsafe and deserve a calm, safety-first response.

Signs to watch for and when it becomes urgent
Look for these clear signs and symptoms during meals:
- Coughing or choking while eating.
- A wet, gurgly voice after swallowing.
- Food “pocketing” in the cheek or prolonged chewing.
- Frequent throat clearing or repeated swallowing attempts.
If a person may choke repeatedly, lose weight fast, become dehydrated, or grow afraid of meals, call a clinician right away. These are safety red flags and a real risk.
Food prep and safe textures
Favor soft, moist foods. Grind or puree when needed. Cut bites small and add sauces or broth to moisten dry items.
Avoid dry, crumbly, or tough foods that scatter in the mouth. Raw carrots, hard candies, and whole nuts are common high-risk foods.
Posture, mouth checks, and caregiver habits
Seat the person upright with feet supported. Keep the head slightly forward. Never tilt the head back during a swallow.
After meals, gently check the mouth for leftover food. Pocketing can lead to choking later and is easy to miss.
Build confidence: learn basic rescue steps like the Heimlich and practice slow, calm feeding. That reduces fear at the table and helps the person keep enjoying eating while living dementia progresses.
| Issue | What you may notice | Simple household fix |
|---|---|---|
| Choking/coughing | Sudden cough, face color change | Stop feeding; assist and seek help if not clearing |
| Wet/gurgly voice | Sounds wet after swallowing | Offer thicker liquids; consult speech therapist |
| Food pocketing | Cheek bulge; slow eating | Smaller bites; check mouth after meal |
| Poor posture | Head tilted back while swallowing | Reposition upright; feet supported, head forward |
“A calm, safety-first approach keeps meals nourishing and less scary.”
Hydration, constipation, and bathroom-related barriers to eating and drinking
Thirst can slip by unnoticed; small sips often work better than big glasses. Offer drinks often, not just at mealtimes. That keeps fluids steady throughout day and eases swallowing.

Offer small drinks and high-water foods
Build simple sip routines tied to the day: after meds, after a walk, during a favorite show. Small cups, juice boxes, and water bottles are easier for pacing.
High-water foods help when plain water is refused: fruit, brothy soups, smoothies, and milkshakes. These support eating and drinking without pressure.
How incontinence fears cut back fluid intake — and what helps
Fears are real: “If I drink, I might not make it.” Validate that feeling. Add clear bathroom signs, night lights, a visible path, or a bedside commode when needed.
Prevent constipation with simple steps
Constipation lowers appetite and raises agitation. Focus on fluids + fiber + movement. Offer portable fiber snacks like yogurt cups or applesauce pouches for restless pacing.
“Hydration plans should lower stress, not cause fights.”
- Reassure caregivers: small, repeated offers beat large amounts.
- Review meds and conditions with the clinician if constipation or low intake persists.
- Keep dignity first—choices, easy cups, and bedside options encourage steady fluid care and better health.
Fix appetite loss and unintended weight loss without turning meals into a battle
When appetite fades, a calm plan beats panic every time. Caregivers often worry, “If they don’t eat, what happens?” Start with small steps you can repeat daily.

Small, frequent meals and nutrient-dense snacks
Offer five to six mini-meals instead of three large ones. Little plates and gentle prompts make food feel less overwhelming.
Choose normal-feeling snacks that pack calories: yogurt cups, smoothies, soft-boiled eggs, nut-butter toast if chewing is safe. These add nutrition without drama.
Favorite foods, pleasant temperature, and flexible preferences
Today’s win matters more than yesterday’s rules. Reheat a favorite meal so it’s comforting. Check temperature before serving—hot or cold can trigger refusal.
When supplements may be recommended
Supplements aren’t automatic. A doctor or dietitian may suggest oral calorie boosts between meals when weight loss continues despite food changes. Think of them as temporary helpers, not a permanent diet swap.
Oral health routines that protect appetite and comfort
Daily mouth care, denture fit checks, and regular dental visits can remove pain that cuts appetite. Dry mouth, sores, or loose dentures often reduce intake—treating those restores comfort and interest in foods.
“Pause, offer again later, and protect the relationship at the table.”
- Keep calm. Skip arguments over plates.
- Try small, nutrient-rich bites often.
- See a clinician if weight loss keeps going or meds may be the cause.
For practical mealtime tips and caregiver resources, see this helpful food and eating guide.
Handle overeating, repeated meals, and unsafe food-seeking behaviors
You might see sudden food-seeking, hoarding, or repeated meal requests that feel confusing. This is common and usually not intentional. Memory gaps, cravings, routine-seeking, boredom, or compulsive oral behaviors can drive it—especially in people with dementia.
Practical portioning and cues:
- Pre-portion snacks in small containers so servings are clear and easy.
- Label containers with a friendly cue like “Next snack at 3:00.”
- Stagger items: show one thing, then remove it before offering the next to slow rapid eating.

Healthy swaps and meaningful activities
Offer low-sugar, high-volume options: fruit, yogurt, applesauce, or steamed veggies with dip. These foods keep fullness without big sugar spikes.
Keep hands and minds busy. Short walks, folding towels, simple music tasks, or cooking helpers reduce food-seeking. These activities are gentle and meaningful.
“They’re seeking comfort and routine—our job is to make it safer.”
| Issue | Quick fix | Why it helps |
|---|---|---|
| Hoarding | Lock high-risk items; pre-portion safe snacks | Reduces access, preserves dignity |
| Repeated requests | Eat together when possible; offer a drink first | Calms routine-seeking, checks blood sugar |
| Compulsive snacking | Swap for fruit or yogurt; add activity | Maintains volume without spikes |
Monitor blood sugar if the person may have diabetes. Above all, respond with warmth and steady care. Small changes protect health and keep mealtimes calmer for people and caregivers alike.
Create a Dementia-Friendly Meal Memory System That Works Even When You Are Not There
For many families, the hardest part of dementia and eating is not preparing the food. It is knowing whether the meal actually happened.
A senior may say, “I already ate,” because they truly believe they did. Another may open the fridge several times, feel unsure what to choose, close it again, and still go without lunch. Someone else may start eating, get distracted, leave the table, and never return to the plate.
This is where families need more than reminders. They need a simple meal memory system.
A meal memory system is a set of visible cues, repeated routines, and caregiver checks that helps the person recognize what meal comes next, where the food is, what step to take, and whether the meal is finished. The goal is not to make the person “remember better.” Dementia often makes that unrealistic. The goal is to make the environment do more of the remembering for them.
This section will help you build that system at home in a calm, respectful, low-pressure way.
Start With One Meal, Not the Whole Day
Trying to fix breakfast, lunch, dinner, snacks, hydration, medication timing, and grocery planning all at once can overwhelm everyone. Start with the meal that causes the most trouble.
For many seniors, lunch is the easiest meal to miss because it often has less structure. Breakfast may happen after waking. Dinner may happen when family calls or visits. Lunch can disappear quietly in the middle of the day.
Choose one target meal and study it for three days.
Ask:
- What time does this meal usually go wrong?
- Is the person alone during that time?
- Is the food already prepared?
- Do they need to heat it?
- Do they know where it is?
- Do they recognize it as “their meal”?
- Do they start eating but stop halfway?
- Do they say they already ate?
- Do they forget how to begin?
Do not change everything immediately. First, find the exact point where the meal breaks down.
If the food is not prepared, the issue is planning. If the food is prepared but not noticed, the issue is visibility. If the food is noticed but not eaten, the issue may be prompting, appetite, confusion, pain, or fatigue. If the person eats but forgets afterward, the issue is confirmation.
Each problem needs a different fix.
Build a “Meal Station” in One Consistent Place
A meal station is a small, predictable area that tells the senior: “This is where food information lives.”
It could be a corner of the kitchen counter, a small table near the dining area, or a section of the fridge door. Keep it simple and uncluttered.
A good meal station may include:
- A large clock.
- A simple whiteboard.
- Today’s date.
- The next meal written clearly.
- One instruction at a time.
- A visible water bottle or cup.
- A small basket for snacks.
- A check-off space for completed meals.
For example:
Today is Tuesday.
Lunch is at 12:30.
Your soup is in the blue bowl in the fridge.
After lunch, tick this box: Lunch done.
This works best when the wording stays calm and familiar. Avoid long notes like, “Please remember that your daughter prepared lunch and you need to eat it before taking your afternoon medication.” That is too much information.
Use short, direct language.
Better:
Lunch: soup + toast.
Heat for 1 minute.
Sit at the kitchen table.
If heating food is unsafe, remove that step. Leave ready-to-eat meals instead, or arrange for a call, visit, or meal delivery around that time.
The meal station should not look like a command center. It should feel like a gentle guide.
Use Clear Food Labels That Answer the Senior’s Real Questions
Many labels fail because they only identify the food. For dementia support, labels should answer the practical questions the person may not be able to organize alone.
Instead of labeling a container:
Chicken
Try:
Lunch for Tuesday
Chicken and rice
Eat at 12:30
Ready to eat
If the person needs help knowing whether something is still safe, add:
Fresh today
Eat today
Do not eat after Wednesday
Use large, dark writing on a plain background. Avoid decorative stickers or busy designs. If vision is poor, use bold marker and high-contrast labels.
Color coding can also help if it is used consistently.
For example:
- Blue sticker = lunch.
- Green sticker = snack.
- Yellow sticker = drink.
- Red sticker = do not touch without help.
Do not use too many colors. Two or three are enough. Too many labels can create more confusion.
If the person tends to eat unsafe leftovers, expired foods, or raw ingredients, simplify the fridge. Put ready-to-eat foods at eye level. Move confusing or unsafe items out of sight. Use a designated “Eat This Today” shelf or clear bin.
The best fridge setup is not the one that stores the most food. It is the one that makes the next safe choice obvious.
Create a Gentle “Before, During, After” Meal Script
Caregivers often repeat reminders in different ways because they are worried. The senior hears multiple versions and may become irritated or embarrassed.
A script keeps everyone consistent.
Use three stages.
Before the meal
The goal is to orient, not pressure.
Try:
“It’s lunchtime now. Your soup is ready on the table.”
If they resist:
“That’s okay. Let’s just sit together for a minute.”
If they say they already ate:
“You may have. I’m not sure either, so I made a small fresh bowl. You can just try a little.”
Avoid:
“You did not eat.”
“You always say that.”
“You have to eat.”
“We talked about this already.”
These phrases may be true, but they usually increase defensiveness.
During the meal
The goal is to keep the next step simple.
Try:
“Here is your spoon.”
“Try one sip.”
“That looks good.”
“Take your time.”
“Would you like another bite or a sip?”
Use pauses. Give the brain time to process.
If they stop eating, gently restart with one cue:
“Here is your toast.”
If they seem overwhelmed, remove extra items from the table and present one food at a time.
After the meal
The goal is confirmation.
Try:
“You had lunch. Nice job. I’ll mark it here.”
Then check the meal off on the board or log. This helps reduce repeat uncertainty later.
If they ask again, point to the visible cue:
“Yes, lunch is done. See, we checked it off. Next is tea at 3.”
This is not about proving them wrong. It is about giving the brain an external anchor.
Use a Meal Completion Log That Does Not Feel Like Surveillance
Families need information, but seniors need dignity. A meal log should feel supportive, not controlling.
Keep it very simple.
Use columns like:
Meal | Offered | Eaten | Drink | Notes
Example:
Breakfast | Oatmeal | Half | Tea | Ate well with music off
Lunch | Soup | Most | Water | Needed one reminder
Snack | Yogurt | All | — | Easy win
Avoid writing judgmental notes such as “refused again” or “being difficult.” Use neutral observations.
Better:
- Turned away after two bites.
- Said mouth felt dry.
- Ate better with smaller spoon.
- Drank more from covered cup.
- Asked for sweet food.
- Seemed tired before meal.
- Coughed twice after water.
- Ate well when daughter called.
This log helps caregivers spot patterns. Maybe breakfast is strong but dinner fails. Maybe meals after bathing are too tiring. Maybe the person eats more when food is warm, soft, or served in a smaller bowl. Maybe water is refused, but tea, soup, melon, or smoothies work better.
Patterns reduce guesswork.
Share the log with a doctor, dietitian, dentist, speech therapist, or home care aide when needed. A clear three-day record is often more helpful than a vague statement like, “She is not eating.”
Match the Reminder to the Person’s Stage of Dementia
Not every reminder works for every stage. A phone alarm may help one person and scare another. A written note may help in early dementia but become meaningless later.
Think in levels.
Level 1: The person can still read and follow simple instructions
Use written meal cards, whiteboards, fridge labels, and phone reminders.
Example:
It is 12:30. Please eat the sandwich on the table.
This works when the person can still connect the instruction with action.
Level 2: The person reads the note but does not act
Add a voice prompt or live call.
Example:
“Hi Dad, it’s lunchtime. Please go to the kitchen table. Your sandwich is on the blue plate.”
Stay on the phone until the first step happens if possible.
Level 3: The person needs help starting
Use step-by-step cueing.
Example:
“Pick up the spoon.”
Pause.
“Take one bite.”
Pause.
“Now have a sip.”
At this stage, the issue is not willingness. It is sequencing.
Level 4: The person cannot safely manage meals alone
Written reminders are no longer enough. Arrange in-person help, supervised meals, texture guidance, swallowing support, or professional care.
Families sometimes continue using reminders long after reminders have stopped working. That can create risk. If meals are consistently missed despite notes, alarms, and calls, it is time to increase support.
Plan for “I Already Ate” Without Arguing
The phrase “I already ate” can mean several things.
It may mean:
- They truly believe they ate.
- They are embarrassed.
- They are tired.
- The plate looks overwhelming.
- They do not recognize the food.
- They are not hungry.
- They are afraid of choking.
- They feel controlled.
- They want the conversation to stop.
Do not treat the phrase as a debate. Treat it as information.
Try a soft reset:
“You may be right. I brought a small snack just in case.”
Or:
“That’s okay. Let’s just have tea and a few bites.”
Or:
“No big meal. Just a little yogurt.”
Small, low-pressure offerings often work better than insisting on a full meal. A few bites repeated throughout the day can protect nutrition without turning eating into a fight.
When possible, avoid asking, “Did you eat?” This question puts pressure on memory.
Ask action-based questions instead:
- “What is on your plate right now?”
- “Can you take a sip while we talk?”
- “Are you sitting at the table?”
- “Is the blue bowl empty or full?”
- “Would you like the soup or the yogurt first?”
These questions help caregivers understand what is actually happening without requiring the person to remember the whole meal.
Make Meals Easier for Seniors Living Alone
When a senior with dementia lives alone, meal support needs to be extremely simple. The system should reduce cooking, reduce choices, and reduce unsafe decisions.
Useful strategies include:
- Ready-to-eat breakfasts.
- Pre-portioned lunches.
- A same-shelf fridge system.
- A daily snack basket.
- Automatic grocery delivery.
- Meal delivery from local programs.
- Family-prepared meals labeled by day.
- A call before or during the highest-risk meal.
- A neighbor or aide check after missed meals.
- Removal of expired or unsafe foods.
Avoid relying on complicated cooking instructions. A note that says “preheat oven, remove film, stir halfway, check temperature” may be too much.
Choose meals that require no cooking or only safe, familiar steps.
Examples:
- Yogurt with fruit.
- Egg salad sandwich.
- Soft cooked vegetables.
- Ready-made soup in a microwave-safe bowl.
- Smoothie in a labeled bottle.
- Cheese and crackers if chewing is safe.
- Oatmeal cup prepared by a caregiver.
- Soft pasta in a clearly labeled container.
- Cut fruit in a clear box.
- Milkshake or nutrition drink if recommended.
If the person leaves the stove on, burns pans, forgets appliances, or eats spoiled food, treat this as a safety issue, not a normal aging issue. Meals may need to shift away from independent cooking.
Use “Food Bridges” When Full Meals Fail
Some days, a full plate will not work. Instead of skipping the meal entirely, use a food bridge.
A food bridge is a small, easy item that gets nutrition into the day and may lead to more eating afterward.
Good food bridges include:
- A few spoonfuls of yogurt.
- A smoothie.
- A banana.
- A small bowl of soup.
- Applesauce.
- Custard.
- Scrambled egg.
- Soft toast with spread.
- A milk drink.
- A small sandwich cut into pieces.
- Warm tea with a snack.
- Pudding with added protein if advised.
The aim is momentum. Once the person starts, they may accept more. Even if they do not, the bridge is still better than a completely missed meal.
Use food bridges when the person is:
- Sleepy.
- Agitated.
- Suspicious.
- Not recognizing the meal.
- Saying they already ate.
- Distracted.
- Restless.
- Overwhelmed by the plate.
A food bridge should be easy to see, easy to hold, easy to chew, and emotionally familiar.
Prepare for Late-Day Appetite Drops
Many seniors with dementia eat better earlier in the day. By evening, fatigue, confusion, and restlessness may increase. If dinner is often difficult, do not wait until dinner to provide most nutrition.
Shift more nourishment earlier.
Try:
- A stronger breakfast.
- A mid-morning snack.
- A protein-rich lunch.
- A calming afternoon drink.
- A smaller, simpler dinner.
- A bedtime snack if appropriate.
This approach reduces pressure on the hardest meal of the day.
For example, if dinner usually becomes stressful, lunch can become the main meal. Dinner can be soup, soft toast, yogurt, or a small familiar plate.
Families sometimes feel dinner “should” be the main meal because that was the old routine. Dementia care often requires flexible routines. The best meal schedule is the one the person can actually follow.
Keep Independence Where It Is Still Safe
A meal memory system should not take over everything too early. Seniors often eat better when they still feel involved.
Offer small, safe roles:
- Choosing between two foods.
- Folding a napkin.
- Stirring a drink.
- Holding a cup.
- Picking the placemat.
- Smelling the soup.
- Buttering soft bread with supervision.
- Carrying a light snack plate.
- Checking off the meal after eating.
These steps preserve dignity. They also help the brain connect with the meal.
Use two-choice questions, not open-ended questions.
Instead of:
“What do you want for lunch?”
Try:
“Would you like soup or a sandwich?”
Instead of:
“What do you want to drink?”
Try:
“Tea or water?”
If even two choices overwhelm them, make the choice yourself and present it warmly:
“I made your tea the way you like it.”
Create an Escalation Plan for Missed Meals
Families should decide in advance what happens when meals are missed. This prevents panic and sibling confusion.
A simple escalation plan may look like this:
One missed meal: Offer a food bridge and fluids. Check mood, pain, bathroom needs, and fatigue.
Two missed meals in one day: Call or visit. Check the fridge, trash, dishes, hydration, medication changes, and signs of illness.
Repeated missed meals across several days: Start a meal log. Contact the doctor, dietitian, or dentist. Review swallowing, mood, constipation, medication side effects, and oral pain.
Missed meals plus red flags: Seek medical advice promptly. Red flags include sudden confusion, dizziness, rapid weight loss, repeated choking, very low fluid intake, dark urine, fever, vomiting, severe constipation, or weakness.
Write this plan down and share it with everyone involved in care.
This is especially important for long-distance caregivers. Without a plan, one family member may assume another checked. A simple system prevents gaps.
Use Calls as Part of the Meal System, Not Just a Reminder
A call can do more than say, “Don’t forget to eat.” It can guide the person through the moment.
A useful meal call might sound like this:
“Hi Mom, it’s lunchtime. Are you near the kitchen?”
Pause.
“Good. Please look for the blue plate on the table.”
Pause.
“What do you see on it?”
Pause.
“That’s your lunch. Take one bite while we talk.”
Pause.
“Great. Now have a sip of water.”
This kind of call confirms location, food visibility, meal start, and hydration. It is more practical than a general reminder.
After the call, the caregiver can note:
- Was food found?
- Did the person begin eating?
- Did they sound confused?
- Did they report pain, nausea, or fear?
- Was there coughing?
- Did they seem lonely or low?
- Is another check needed?
For seniors who do not use smartphones or apps, phone-based support can be easier than digital notifications. A familiar voice, calm pacing, and simple prompts can help the meal actually happen.
Review the System Every Two Weeks
Dementia changes over time. A system that works now may need adjusting later.
Every two weeks, ask:
- Which meal is still being missed?
- Which cue is no longer working?
- Is the person eating less overall?
- Are they coughing more?
- Are they losing weight?
- Are they drinking enough?
- Are they more suspicious of food?
- Are labels still helpful?
- Is cooking still safe?
- Does the caregiver need more help?
Do not see these changes as failure. They are signals that the care plan needs to match the person’s current abilities.
The most helpful approach is steady, flexible, and kind. Make the next right action easier. Remove unnecessary decisions. Use visible cues. Confirm meals without shame. Bring in support before the situation becomes a crisis.
A senior with dementia may not always remember the meal, but with the right system, they can still be guided toward nourishment, comfort, and dignity.
How Caregivers Can Know When Meal Problems Need More Support
Many families start with small fixes: a reminder note, a phone call, a labeled lunch box, a favorite snack, or a calmer dining table. These steps can make a real difference. But dementia changes over time, and eating problems can quietly move from “manageable at home” to “needs more support.”
This is one of the hardest parts for caregivers. You may wonder: Is this just a bad day? Is Mom being picky? Is Dad safe alone at lunchtime? Should we call the doctor? Do we need a home aide? Are we overreacting?
The goal is not to panic over every missed snack. The goal is to notice patterns early, respond calmly, and add the right level of help before weight loss, dehydration, choking, or unsafe kitchen habits become serious.
A good care plan should answer three questions:
- Is the person getting enough food and fluids most days?
- Can they eat safely without confusion, choking, or risky kitchen use?
- Is the current support system realistic for the caregiver?
If the answer to any of these is “not anymore,” it may be time to adjust the plan.
Look for Patterns, Not One-Off Moments
Everyone has days when they eat less. Seniors may skip a meal because they feel tired, constipated, lonely, nauseated, or simply not hungry. One light meal is not always an emergency.
What matters more is the pattern.
Watch for changes such as:
- Skipping the same meal several days in a row.
- Losing interest in foods they used to enjoy.
- Leaving plates untouched but saying they ate.
- Eating only sweets, toast, tea, or very small snacks.
- Drinking much less than usual.
- Becoming weaker, sleepier, or more unsteady.
- Needing more reminders than before.
- Forgetting how to start eating.
- Coughing, pocketing food, or sounding wet after swallowing.
- Letting food spoil in the fridge.
- Reheating the same food repeatedly.
- Leaving the stove, kettle, or microwave unattended.
A pattern gives you useful information. For example, if breakfast is fine but dinner fails, the person may be more confused or tired later in the day. If lunch is missed only when they are alone, the issue may be lack of cueing. If they refuse meat but accept soup, yogurt, eggs, or smoothies, chewing or denture discomfort may be involved.
Try not to label the behavior too quickly. “Picky,” “stubborn,” or “difficult” can hide the real cause. A better question is: What ability has changed, and what support would make eating easier?
Use a Three-Day Meal Reality Check
Before making big changes, do a simple three-day review. This gives families a clearer picture and helps doctors, dietitians, or home care providers give better advice.
For three days, write down:
- What time food was offered.
- What food was offered.
- How much was eaten.
- How much fluid was taken.
- Whether the person needed reminders.
- Whether they ate alone or with someone.
- Any coughing, choking, pocketing, pain, or refusal.
- Mood before the meal.
- Energy level after the meal.
- Any bathroom issues, constipation, or signs of dehydration.
Keep the notes brief. You do not need a perfect food diary. You need enough detail to see what is really happening.
For example:
Monday lunch: Chicken soup and toast. Ate half with one reminder. Drank small glass of water. No coughing. Seemed tired.
Tuesday lunch: Sandwich on table. Untouched after two hours. Said she already ate. Drank tea only.
Wednesday lunch: Yogurt and banana during phone call. Ate all yogurt, half banana. Needed step-by-step prompting.
This tells you something important: a full meal left alone may not work, but a smaller meal with a live prompt may work well.
That is useful. It shows the person may not need a completely different diet yet. They may need better timing, simpler food, and active cueing.
Decide What Kind of Support Is Missing
Meal problems usually fall into one of four support gaps.
1. Memory support gap
The person can eat safely, but they forget the meal exists or believe they already ate.
Helpful support may include:
- Scheduled phone calls.
- Visual meal boards.
- Labeled food containers.
- A daily checklist.
- A caregiver confirmation after meals.
- A service that checks in at mealtime.
This stage is often where structured reminders work well.
2. Initiation support gap
The person sees the food but does not begin eating. They may stare at the plate, move food around, or get distracted.
Helpful support may include:
- Sitting with them for the first few minutes.
- Giving one-step prompts.
- Offering one food at a time.
- Starting with a small bite or sip.
- Modeling the action by eating beside them.
- Using finger foods or easier utensils.
At this point, a note may not be enough. The person may need someone to help start the sequence.
3. Physical comfort support gap
The person wants to eat but pain, dry mouth, swallowing difficulty, constipation, fatigue, or medication side effects get in the way.
Helpful support may include:
- Dental review.
- Medication review.
- Softer, moister foods.
- Constipation management.
- Swallowing assessment.
- Dietitian guidance.
- Smaller, more frequent meals.
This is where families should avoid guessing for too long. If the body is making eating uncomfortable, reminders alone will not solve the problem.
4. Safety support gap
The person cannot safely manage meals alone. They may choke, leave appliances on, eat spoiled food, forget to turn off the stove, or become confused with hot liquids.
Helpful support may include:
- Supervised meals.
- Removing unsafe appliances.
- Ready-to-eat meals only.
- In-home care visits.
- Meal delivery with check-ins.
- Occupational therapy home safety review.
- A higher level of daily caregiving.
This is not about taking independence away. It is about preventing harm while keeping as much dignity and choice as possible.
Know When a Reminder Is No Longer Enough
Families often continue using reminders because reminders feel respectful and non-invasive. That makes sense. Nobody wants to overstep.
But reminders only work when the person can still understand the reminder, connect it to an action, and complete the action safely.
A reminder may no longer be enough if:
- The person turns off alarms without eating.
- Notes are ignored or misunderstood.
- They say “yes, I ate” but food is untouched.
- They cannot find the labeled meal.
- They become anxious or annoyed by repeated prompts.
- They start eating but stop after one or two bites.
- They forget how to use utensils.
- They cough or choke during meals.
- They use unsafe appliances despite warnings.
- They need someone to physically guide the meal.
When this happens, do not simply add more reminders. Too many reminders can feel like nagging and may increase frustration.
Instead, change the type of support.
For example:
- Move from written notes to voice calls.
- Move from voice calls to live mealtime companionship.
- Move from independent reheating to ready-to-eat meals.
- Move from large meals to smaller guided snacks.
- Move from occasional family checks to scheduled daily support.
The question is not, “How do we make them remember?” The better question is, “What support removes the need to remember?”
Create a Family Mealtime Responsibility Plan
Meal care often becomes stressful because everyone assumes someone else is watching the situation. One sibling may think a parent is eating because the fridge has food. Another may assume a neighbor is checking. A spouse may be too exhausted to report every skipped meal.
A written family plan prevents gaps.
Include:
- Who checks breakfast.
- Who checks lunch.
- Who checks dinner.
- Who handles groceries.
- Who reviews the fridge.
- Who books doctor or dental appointments.
- Who tracks weight.
- Who responds if meals are missed.
- Who pays for meal delivery or care support.
- Who receives updates from check-in calls or aides.
Keep the plan realistic. A long-distance caregiver may not be able to visit daily, but they can schedule calls, review reports, order groceries, arrange meal delivery, or coordinate appointments. A nearby relative may handle fridge checks and in-person visits. A paid aide may cover the most difficult meal of the day.
The plan should also include a backup person. If the usual caregiver is sick, traveling, or overwhelmed, someone else should know what to do.
Set Clear Action Triggers
Caregivers should not have to make every decision from scratch. Action triggers help families respond quickly and consistently.
Examples:
If one meal is missed:
Offer a small snack, drink, or favorite food later. Check whether the person is tired, constipated, upset, or in pain.
If two meals are missed in one day:
Call or visit. Check the fridge, trash, dishes, hydration, and medication routine. Offer easy food and fluids.
If meals are missed repeatedly for three days:
Start a meal log and contact a doctor, dietitian, or care professional for guidance.
If there is coughing, choking, wet voice, or food pocketing:
Pause the meal and ask for medical or swallowing guidance.
If there is rapid weight loss, dizziness, weakness, sudden confusion, very low urine, fever, vomiting, or severe dehydration signs:
Seek medical help promptly.
If unsafe cooking happens more than once:
Change the kitchen setup. Remove or disable risky appliances, switch to ready-to-eat meals, and arrange more supervision.
These triggers reduce caregiver guilt because the family is not “guessing.” They are following a care plan.
Protect the Caregiver From Burnout
Eating problems can become emotionally heavy. It is painful to watch someone you love refuse food, forget meals, lose weight, or become upset at the table. Caregivers may feel responsible for every bite.
But no one can monitor meals perfectly all day, every day, without support.
Caregiver burnout can show up as:
- Dreading mealtimes.
- Feeling angry or helpless.
- Arguing about food more often.
- Losing sleep over missed meals.
- Checking constantly but still feeling unsure.
- Skipping your own meals or rest.
- Feeling guilty when you are not there.
If this is happening, the care plan needs to support both people. A senior’s nutrition matters, and the caregiver’s health matters too.
Helpful changes may include:
- Scheduling one daily check-in call.
- Asking another family member to own one meal.
- Using meal delivery.
- Hiring help for lunch or dinner.
- Preparing foods in batches.
- Keeping a shared meal log.
- Asking a doctor for a nutrition referral.
- Joining a dementia caregiver support group.
- Using respite care when needed.
Support is not a sign that you are failing. It is how dementia care becomes sustainable.
Keep the Senior Involved in Decisions When Possible
Even as dementia progresses, many seniors still respond well to respect, choice, and familiar routines. Meal support should not feel like a loss of control.
Use language that protects dignity.
Instead of:
“You can’t cook anymore.”
Try:
“Let’s make lunch easier and safer, so you do not have to fuss with the stove.”
Instead of:
“You keep forgetting to eat.”
Try:
“We’re setting up a simple lunch routine so the day feels easier.”
Instead of:
“You need someone watching you.”
Try:
“Someone will stop by around lunch so you have company.”
Whenever possible, offer small choices:
- “Would you like soup or eggs?”
- “Would you rather eat at the table or by the window?”
- “Tea before lunch or after?”
- “Blue cup or white cup?”
- “Would you like music off or soft music on?”
Small choices preserve personhood. They also reduce resistance because the senior still has a voice in the routine.
Review the Plan as Dementia Changes
A meal care plan is not permanent. It should change as the person’s needs change.
Review the plan every month, or sooner if there is a noticeable decline.
Ask:
- Is the person still eating enough?
- Are reminders still working?
- Are meals taking much longer?
- Is chewing or swallowing harder?
- Are they losing weight?
- Are they drinking enough?
- Is the kitchen still safe?
- Is the caregiver coping?
- Does the person need more companionship at meals?
- Is it time for professional input?
Sometimes the right adjustment is small: a different cup, softer food, clearer labels, or a better call time. Sometimes the adjustment is bigger: supervised meals, in-home help, or a safer living arrangement.
The key is to respond early. Waiting until a crisis can make decisions rushed and emotionally harder.
The Main Goal: Safe Nourishment With Less Stress
Dementia can make eating unpredictable, but families do not have to handle every missed meal with panic. A practical support plan turns worry into action.
Start by observing patterns. Use a simple meal log. Identify whether the issue is memory, initiation, comfort, or safety. Add the right support at the right time. Keep the senior involved wherever possible. Protect the caregiver from carrying the entire routine alone.
Most importantly, remember that food is not only nutrition. It is comfort, rhythm, identity, and connection. Even when memory changes, a calm voice, a familiar meal, a safe table, and a kind routine can still help a senior feel cared for.
The aim is not a perfect plate every time. The aim is steady nourishment, fewer risks, and more peaceful mealtimes for everyone involved.
Daily routines and support systems that reduce missed meals
Use predictable mealtimes, reminders, and visual prompts
Set the same time for breakfast, lunch, and snacks each day. A simple weekly menu cuts choice and keeps the person calm.
Practical prompts: phone alarms, notes on the fridge that say “Lunch at 12,” and one-line scripts like, “It’s lunchtime—your soup is in the fridge.” These reminders help without nagging.
Safety-minded kitchen habits for decreased judgment
Decreased judgment can leave the stove on or timers ignored. Use automatic shut-off appliances and unplug small devices after use.
Label timers with sticky notes and favor microwave-safe, low-effort options. Consider an occupational therapist for a kitchen safety assessment.
Community and at-home support options
Meal delivery services, including Meals on Wheels, bring fresh food and steady support. Local food programs often deliver produce and help with shopping.
Caregiver check-ins and JoyCalls for peace of mind
Set it and support it: scheduled reminders, a friendly call, and quick alerts to you when patterns change.
- Daily check-in calls help prompt mealtimes and hydration.
- Caregivers get summaries and alerts if a person misses meals or shows mood shifts.
“A short, kind reminder can protect health and preserve dignity.”
Sign up for JoyCalls: Sign up for JoyCalls — or Talk to Joy now: 1-415-569-2439. For timing tips and whether morning or evening calls work best, see our guide on morning vs. evening check-ins.
Conclusion
Simple, repeated steps at the table can restore comfort for many older adults.
In short, dementia may change how a person approaches food, but calm routines, one-item servings, and steady hydration protect health and dignity.
Watch for red-flag signs and rule out medical causes before changing a plan. Keep favorites, offer gentle cues, and choose calm over conflict.
Progress will vary. Some days improve and some need new tweaks. You are not failing—this is hard, and you are showing up.
Practical next step: if you need regular check-ins, Sign up for JoyCalls: https://app.joycalls.ai/signup or Talk to Joy now: 1-415-569-2439.